In the first two parts of our series on the immune system, we covered cell-mediated immunity and humoral immunity — essentially, the whole range of immune cells (T-cells, B-cells, macrophages, etc. plus antibodies). Now, we start picking up the odds and ends, including:
- The complementary immune system
- How your immune system communicates
- How we build immunity
Understanding each of these aspects of the immune system offers you an opportunity to fine tune performance and enhance your resistance to disease.
The Complementary Immune System
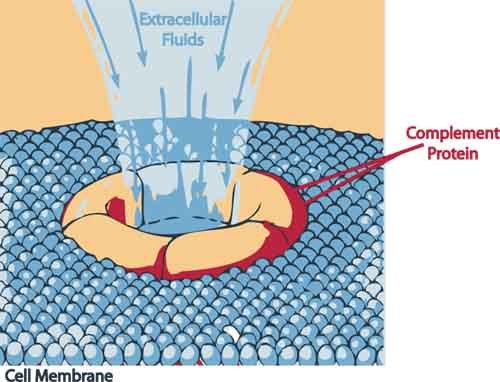
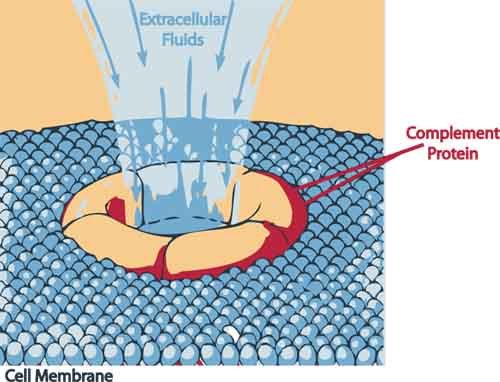
If the initial cell-mediated immune response is overwhelmed, the “complementary immune system” (aka, the complement system) kicks in. The complement system helps or “complements” the ability of antibodies and phagocytic cells to clear pathogens from your body. This secondary system is comprised of approximately twenty-five proteins and enzymes that activate in a cascading sequence and end with what’s called the “membrane attack complex.” As its name implies, the membrane attack complex attacks the cell walls of invaders — literally blowing holes in them.
The different proteins and enzymes of the complement system are generally synthesized by the liver. When stimulated, the complement system cleaves to antibodies that have attached themselves to the surfaces of invading and/or mutant cells. Once “cleaved,” they release cytokines, which initiate a cascade of further cleavages and further cytokine releases that:
- Attract even more immune cells to attack the invaders.
- Increase vascular permeability, which enhances the ability of immune cells to reach the invader.
- Mark the pathogens for destruction by the immune system.
- And as a bonus, some of the proteins and enzymes released as part of the complement cascade can actually kill unwanted cells directly by blowing apart their cellular membranes.1 Rus H, Cudrici C, Niculescu F (2005). “The role of the complement system in innate immunity”. Immunologic Research 33 (2): 103–12 <http://www.springerlink.com/content/d576088500r3x442/>
A secondary function of the complementary immune system is to help rid the body of Circulating Immune Complexes (CIC’s). CIC’s start out as extra-large protein molecules (primarily from wheat, corn, and dairy) that are only partially digested in the small intestine and then absorbed into the bloodstream. Once in the bloodstream, the immune system treats them as invaders because they are too large to be metabolized, thus provoking an immune reaction. Antibodies couple with these foreign protein invaders to form CIC’s. At first, these CIC’s may be neutralized by phagocytes in the lymphatic system and subsequently flushed out of the body through the lymph system. But over time, as you continue to eat more and more of the offending foods, too many CIC’s are created, and they overwhelm the body’s ability to eliminate them. In addition, they overwhelm the immune system, and they overwhelm your kidneys. At this point, your body has no choice but to “store” them somewhere in the hope that it can deal with them later. For lack of a better option, it stores the CIC’s in its soft tissues — muscles, organs, you name it. Unfortunately, your immune system can still sense the antigens in the CIC’s even though they are buried in your soft tissue and continues to attack them as invaders. And even more unfortunately, your immune system cannot separate the antigens in the CIC’s from the soft tissue in which they are stored– so it attacks both. In effect, your body is now attacking itself. This leads directly to chronic, systemic tissue inflammation and, ultimately, autoimmune disorders.
It is here that a good proteolytic enzyme formula can come into play. Proteolytic enzymes can compensate for your unhealthy dietary choices by making their way into your bloodstream, where they get to work breaking down CIC’s in your blood and soft tissue — eventually passing the waste out through your kidneys. Not only can this relieve the autoimmune condition caused by the stored CIC’s, but it also takes huge stress off your immune system, freeing it up to focus on real invaders.
How Your Immune System Communicates
We now have a sense of how the immune system works and how it identifies invaders and mounts a response, but how does it communicate with itself? The answer lies in the powerful cytokine chemical messengers secreted by the cells of the immune system that we discussed previously. These include interferon and tumor necrosis factor (TNF), but it is the interleukins in particular that swarm through the body like billions of tiny messengers. They activate the B-cells and T-cells, “train” cells as to what enemies to fight, and promote the rapid growth of “intelligent” defenses. They also shut down defenses when the threat is gone and control the inflammation response. In short, they provide a remarkable set of intelligent checks and balances on the immune system — guiding it, training it, regulating it, marshaling it as required, and resting it when no longer needed. And as we learned in our last newsletter, some natural immune boosters, such as suma and astragalus work by boosting cytokine production — which leads right into a discussion of how we build immunity.
How We Build Immunity
When we are born, we have weak immune systems. Whatever immunity we have is given to us by our mothers. Almost immediately, however, if we are nursing, that immunity begins to grow. The first “milk” we receive from our mothers is, in fact, not actually milk but a substance called colostrum, whose primary purpose is to boost our immunity. Colostrum is packed with natural immune boosters, such as immunoglobulins, lactoferrin, alkylglycerols, and transfer factor. In addition, nursing helps build the cultures of “friendly bacteria” in the digestive tract, which also support immune function. Children that are put on formula are denied these benefits. Not only are formula-fed children more liable to experience colic, ear infections, and colds, but there is significant evidence that their immune systems never fully “catch up” no matter how hard they try to build them later.
The primary way we build immunity is by “teaching” our immune systems how to respond more quickly and more aggressively. Whenever T-cells or B-cells become activated by an invader, some of those cells become memory cells — they encode a “memory” of the particular antigen associated with that invader so that the next time they encounter the same antigen, the immune system can respond without delay. In other words, having an illness and being exposed to microbes on a daily basis trains the body to better defend against that illness and those microbes the next time they appear. That said, there are a number of factors that affect the level of immune response we are capable of mounting. Genetics certainly plays a role, as some individuals are born with stronger immune systems than others. Diet, lifestyle, and environment can also enhance or erode the immune system. Zinc for example is essential for a healthy immune system as it helps to increase the levels of T-Cells and white blood cells in our body. Likewise, selenium is also essential, again being required for white cell production. Thus, a diet deficient in either zinc or selenium will produce a less than optimal immune system. In addition, the strength of your immune response and the duration of your immune memory of an invader are strongly influenced by the type of antigen that was detected and how much of it originally entered the body. This becomes important when we consider the efficacy of vaccination.
In truth, we actually build immunity in five different ways:
- Active immunization happens when your body is presented with something that it considers “non-self.” This can be either a foreign invader, or a newly formed cancer cell. Your body then mobilizes its immune system (either cell-mediated or humoral) in response to the invader. Exposure to measles, mumps, and chickenpox as a child, for example, can provide immunity for many years — in some cases, for the rest of your life.
- Specific immunization involves the injection of a reduced-strength antigen into the blood to enable the body to then produce its antibodies. The other word for this, of course, is vaccination.
- Nonspecific immunization is different in that it involves the injection of certain antigens that raise the level of immune function throughout the body — but against an entirely different invader than is presented by the antigen itself. The common acne bacterium, Corynebacterium parvum, is an example. The use of C. parvum as an immunoadjuvant seems to have the ability to stimulate the immune system so as to inhibit tumor growth throughout the body.2 HOLGER KIRCHNER, MOSHE GLASER & RONALD B. HERBERMAN. “Suppression of cell-mediated tumour immunity by Corynebacterium parvum. Nature 257, 396 – 398 (02 October 1975). <http://www.nature.com/nature/journal/v257/n5525/abs/257396a0.html> Bacille Calmette-Guerin (BCG), on the other hand, is the only effective vaccine for protection against tuberculosis,3 “BCG – the current vaccine for tuberculosis.” Initiative for Vaccine Research (IVR). World Health Organization. Accessed 7 Sept 2011. <http://www.who.int/vaccine_research/diseases/tb/vaccine_development/bcg/en/> an entirely different pathogen. And as we discussed in our last newsletter, some natural immune boosters such as Echinacea work in a similar way, by tricking the immune system into building up its defenses in general. And since there is no real invader requiring the use of these defenses, they can lie in wait, perpetually ready for the appearance of a real invader.
- Adopted immunotherapy requires the direct injection of, typically, interleukin-2 to stimulate the immune system. Some immune boosters such as suma and astragalus, again as we discussed last issue, work by stimulating cytokine production.
- Passive immunization is defined by the active infusion of antibodies against a specific disease or invader, either by direct injection or through the womb. No memory or build-up is required. The injection of gamma globulin, for example, will kill Hepatitis A for about 6 months before it is used up. Natural pathogen destroyers, which we will talk about later, fall into this category.
| Active and Passive vs. Specific and Non-specific Immunity | ||
| Active Immunization |
Passive Immunization |
|
| Specific | Exposure to measles, mumps, and chickenpox as a child
Smallpox vaccine Killed melanoma cells Hepatitis B Vaccine Oral Polio Vaccine |
Pooled gamma globulin against Hepatitis ANatural pathogen destroyers Natural antibodies passed |
| Non-Specific | Corynebacterium Parvum
BCG Echinacea like immune boosters |
Adoptive immunotherapy with IL-2 incubated with lymphocytes against cancerSuma and astragalus like immune boosters |
Before we continue, we need to repeat something that we discussed in the first part of our series — exactly how immunity works. Consider the example of a mother taking care of her child with measles. How does her previously acquired immunity prevent her from getting measles? The thing of it is: it actually doesn’t. Virtually every mother exposed to the measles by her child catches those same measles from her child no matter how many times she’s been vaccinated or had measles herself. But because of her immune system’s “memory” of measles, her immune system’s response is so fast that she totally eradicates the invader before she even gets one single symptom — assuming, of course, that the memory of the antigen is still strong enough and that her immune system is capable enough. This is a really, really important point to understand about your immune system. Even if you have immunity, you’re still going to get the disease, if the virus or bacteria enters your body. The virus absolutely starts reproducing in your body, but the response is (or can be) so fast that it kills the virus before it can ever really get started. It’s gone before you ever even knew it was there. That’s how immunity works. But it’s not only the speed of the response that’s increased, it’s also the strength. The response triggered by memory cells during second exposure to an invader can be as much as a 1000 times stronger than the initial response. And that’s how a trained immune system can protect you against a foreign invader — virus, bacteria, fungus, whatever. But it also explains why vaccines do not necessarily offer complete protection — nor, for that matter, does actually getting the disease naturally in all cases guarantee protection. Then again, even if the immunity is not perfect and you get the disease, if there is any memory of the disease in your immune system, the likelihood is that there will at least be enough protection to minimize the extent and severity of infection — which, in some cases, might be just enough to save your life.
Vaccines
In the wisdom of modern medicine, we have created vaccines to “pre-build memory” for our immune systems — memories of significant diseases we have never had such as measles, mumps, polio, diphtheria, and smallpox. Vaccines contain a weakened, sterilized version of microorganisms (or proteins from those microorganisms) that is capable of producing an immune response in the body without inducing a full-blown onset of the disease itself. Although vaccines have played a significant role in helping reduce the number of deaths among children, this benefit has not come without cost.
I understand that vaccines are an emotional issue for many people. Whenever the Foundation has published anything that even hints that vaccines might be even slightly beneficial, the response from some of our members has been fast and furious. They don’t like it and call me out as a traitor to the cause. For many of our readers, the only good vaccine is a dead vaccine. However, it is not the role of the Foundation to automatically support all positions prevalent in the alternative health community. Our role is to offer reasoned, balanced, health advice — no matter where it leads. So that said, the truth about vaccines is that:
- They are not as effective as the medical community and the media promote.
- Nor are they as safe as promised.
- On the other hand, they are not as ineffective as many in the alternative health community believe.
- Nor quite as dangerous.
Let’s examine these statements one at a time:
1. Vaccines are incredibly effective — not necessarily
Now that you actually know how the immune system works, we can actually explore in some detail how vaccines work and why they might not always work as well as promised.
 Because the vaccination uses only a weakened version of the invader, or even a partial protein fragment, the memory of the disease left behind in your immune system might not be that strong (not enough memory cells) to initiate an effective response when the invader returns at a later date.
Because the vaccination uses only a weakened version of the invader, or even a partial protein fragment, the memory of the disease left behind in your immune system might not be that strong (not enough memory cells) to initiate an effective response when the invader returns at a later date.- Your immune system might be too compromised when you get the vaccination so that it is unable to fully respond to the antigen — thus leaving a weakened defense in place.
- Then again, vaccines are only as effective as your immune system is when the invader returns. If your immune system isn’t very strong, even if told by your “vaccinated memory” in plenty of time that an old enemy has returned, your immune system just might not be capable of ramping up a strong response in a short period of time. For example, if your immune system is preoccupied battling Circulating Immune Complexes, it might succumb to a new infection of measles. Or if it’s been compromised by an HIV infection, it may not be able to muster a defense against tuberculosis, even if you’ve been vaccinated.
- A vaccine is only as good as the antigen included in it. That means, that when it comes to flu vaccines, for example, they are all based on previous years’ strains of flu — because those are the only antigens available to use. If this year’s strains are different, you’re out of luck. And in fact, although the medical community bills flu vaccines as de rigueur, and 90% effective, they are not — not even close. In truth, the cohort studies that every doctor bases their assessment on are essentially nonsensical. If you were to take them at face value, you would have to conclude that flu vaccines also protect you from lightning strikes, muggings in alleys, and death from terrorist attacks. Obviously, the information contained in these studies is not useful. And yet doctors and governments promote the expenditure of billions and billions of dollars every year on them, despite all evidence to the contrary. Another example of the importance of the antigen being used would be the measles vaccine. The measles circulating today might have enough genetic differences from the one you were inoculated against that your original vaccination, or even having the disease as a child, might no longer offer any protection.4 Charles Arthur, Technology Editor. “New strains of measles may resist vaccination.” 12 April 2001. Vaccination News. Accessed 9 Sept 2011. <http://www.vaccinationnews.com/Rally/NewMeaslesResist.htm>
- Some vaccines trigger long term memory cell responses, but others much less so.
- Rabies vaccine is good for about two years.
- Tetanus, 10 years.
- Measles — potentially life long.
The bottom line is that although all vaccines will trigger some degree of immune response, in some cases, and in some people, that response may be less than promised. Correspondingly, exposure to the actual disease is likely to produce a stronger and more long lasting immune response than a vaccination, but it too offers no absolute guarantees. Or to put it another way: both having measles as a child or getting a vaccination will provide protection from later infection — but neither guarantees that you won’t get measles later, although if you do, the intensity of the infection is likely to be reduced.
2. They are perfectly safe — again, not necessarily
 I’m not going to dwell on this issue, because, as I have explained on different occasions, I have a strong emotional attachment to it, which makes it impossible for me to be objective. My youngest brother was one of those “small percentage” of children who responded badly to the series of three immunization shots he received back in the early 1960s. Each time he received one of the shots, he ran a high fever and cried all night, the last time literally screaming for several hours. Each time, my mother called the pediatrician, who reassured her that it was nothing to worry about. As it turns out, the doctor was wrong: my brother, along with thousands of other children, had an allergic reaction to the shots. Each shot caused a small brain hemorrhage, ultimately leaving him severely retarded. Although the manufacturer of the vaccine had indications that this was a possibility, they had not made it clear to the pediatricians who used it. Also, before 1990, doctors were not legally obligated to report adverse reactions to vaccines to the U.S. Centers for Disease Control (CDC); and even with the current legal obligation, it’s estimated that only 10 percent of doctors report the damage they see to the CDC.
I’m not going to dwell on this issue, because, as I have explained on different occasions, I have a strong emotional attachment to it, which makes it impossible for me to be objective. My youngest brother was one of those “small percentage” of children who responded badly to the series of three immunization shots he received back in the early 1960s. Each time he received one of the shots, he ran a high fever and cried all night, the last time literally screaming for several hours. Each time, my mother called the pediatrician, who reassured her that it was nothing to worry about. As it turns out, the doctor was wrong: my brother, along with thousands of other children, had an allergic reaction to the shots. Each shot caused a small brain hemorrhage, ultimately leaving him severely retarded. Although the manufacturer of the vaccine had indications that this was a possibility, they had not made it clear to the pediatricians who used it. Also, before 1990, doctors were not legally obligated to report adverse reactions to vaccines to the U.S. Centers for Disease Control (CDC); and even with the current legal obligation, it’s estimated that only 10 percent of doctors report the damage they see to the CDC.
This sort of reaction to a vaccine and this sort of irresponsibility by a pharmaceutical company are not as anomalous as you might think. The polio vaccine given to children in the 1950s and 1960s was not as sterilized as originally thought. In fact, when better test equipment was later used, it was found that there were over 140 live viruses in early versions of the vaccine. One of those viruses, SV40, is strongly implicated in brain cancer. Jonas Salk testified before a U.S. Senate subcommittee that, since 1961, except for a few importations from other countries, all cases of polio were caused by the oral polio vaccine. In fact, there is strong evidence that the original polio epidemic itself in the late 1940s was caused (or at least greatly exacerbated) by another vaccine. The early triple vaccine against diphtheria, whooping cough, and tetanus has been shown beyond doubt to cause paralytic polio in some children. The incidence of polio in children vaccinated with this shot was statistically greater than in unvaccinated children. This scandal broke in Britain during 1949, an epidemic year for polio; other reports soon followed from Australia.
And there is another problem. In the old days, pharmaceutical companies merely used the viral and bacterial antigens and DNA that nature provided as the basis of their vaccines. But that’s so yesterday! Today, thanks to the science of genetic engineering, vaccine manufacturers can make their own viral DNA from scratch. Very simple. Very clean. Except if they get it wrong and accidentally introduce an active “unnatural” form of the viral DNA into the vaccine — as appears to have happened with the HPV vaccine, Gardasil.5 Leslie Carol Botha. “SANE Vax Inc. Discovers Potential Bio-hazard Contaminant in Merck’s Gardasil™ HPV 4 Vaccine.” 12 September 2001. Sane Vax, Inc. Accessed 14 Sept 2011. <http://sanevax.org/sane-vax-inc-discovers-potential-bio-hazard-contaminant-in-merck%E2%80%99s-gardasil%E2%84%A2-hpv-4-vaccine-2/>
The bottom line is that vaccines are not “perfectly” safe.
3. They are totally ineffective — again, not necessarily
 There are two arguments I hear from the alternative health community in this regard. First, people will tell me of their own experience: they were vaccinated and still came down with the disease later. Ipso facto: vaccinations don’t work. But it’s never a good idea to generalize from a single person’s experience. As we’ve already discussed, there can be several reasons as to why the vaccination didn’t work — including the fact that although it didn’t stop you from getting the disease, it may have reduced its severity. Also, as we’ve already discussed, getting the disease naturally doesn’t “totally” guarantee protection.
There are two arguments I hear from the alternative health community in this regard. First, people will tell me of their own experience: they were vaccinated and still came down with the disease later. Ipso facto: vaccinations don’t work. But it’s never a good idea to generalize from a single person’s experience. As we’ve already discussed, there can be several reasons as to why the vaccination didn’t work — including the fact that although it didn’t stop you from getting the disease, it may have reduced its severity. Also, as we’ve already discussed, getting the disease naturally doesn’t “totally” guarantee protection.
The other argument is more interesting. And that is that infectious diseases have their own natural ebb and flow, which leads to the conclusion that mass vaccination did not help make a disease recede; it was merely the result of the disease’s natural ebb, along with improvements in nutrition, better living standards, and public and personal sanitation.6 GordonT. Stewart. “VACCINATION AGAINST WHOOPING-COUGH : Efficacy versus Risks.” Volume 309, Lancet. Issue 8005, 29 January 1977, Pages 234-237 <http://www.sciencedirect.com/science/article/pii/S0140673677910285> ,7 Roman Bystrianyk. “The Vaccine War: A Forgotten History.” 28 April 2010. I. http://www.healthsentinel.com/joomla/index.php?option=com_content&view=article&id=2752:the-vaccine-war-a-forgotten-history&catid=5:original&Itemid=24 And there is truth to this argument. Both smallpox and polio, for example, were ebbing before vaccinations were introduced. On the other hand, there is a significant statistical correlation between the introduction of these vaccines and the countries where that ebbing was most pronounced. Also, ebb and flow do not explain the disappearance of smallpox as a disease from the face of the earth.
Whatever the flaws in the effectiveness of vaccines, they are not totally ineffective. Even the flu vaccine, which may have only a marginal ability to prevent the flu, probably plays a significant role in lessening the intensity of the flu if you do get it. If you are very old or have a compromised immune system, this may be enough of a difference to save your life.
4. They cause widespread harm — sort of yes, sort of no
It all depends on how you define widespread. In fact, the incidence of serious side effects is low, at least officially. According to the CDC, only about one in 10,000 children have a serious reaction to the standard childhood vaccines, such as lowered consciousness, coma, swelling inside the mouth, difficulty breathing, low blood pressure, central nervous system conditions including encephalitis and encephalopathy, and anaphylactic shock. About 20%, however, have so-called “minor” reactions, which can include extensive rashes and fevers of greater than 103 F (39.4 C).8 Update: Vaccine Side Effects, Adverse Reactions, Recommendations and Reports. “Contraindications, and Precautions Recommendations of the Advisory Committee on Immunization Practices (ACIP).” CDC September 06, 1996 / 45(RR-12);1-35. <http://www.cdc.gov/mmwr/preview/mmwrhtml/00046738.htm>
So what do these numbers mean?
First, let’s pretend that governments have never lied to us to promote a given agenda (can you say Gulf of Tonkin, weapons of mass destruction, and swine flu vaccine) and that these numbers are accurate. What do they mean? When you consider how many children are vaccinated each year, year after year, that comes out to tens of millions of children in the US alone. One in 10,000 when applied to 50,000,000 children, that works out to some 5,000 children who have suffered life-compromising side effects over the past few decades and 10,000,000 who have suffered severe rashes, profound body ache, high fevers, and whatnot — in the United States alone.
So do vaccines cause widespread harm? Statistically no, but mathematically yes! And if you happen to be the parent of a child like my little brother who suffered massive brain damage as the result of vaccination, then statistics and mathematics really don’t matter, do they? It’s been 24 years since my little brother passed away, and like Mr. Bojangles, I still grieve.
In 1986, the U.S. government set up a National Vaccine Injury Compensation Program to compensate those harmed by vaccines. To date, over $1.5 billion has been paid out.
But if vaccines really do prevent epidemics of whooping cough, diphtheria, smallpox, and polio –or lessen their severity — are the “statistically” rare victims like my brother too high a price to pay? In the end, each parent needs to make that call for themselves.
Conclusion
I know I’ve entered a hornets’ nest by even suggesting that there might be any conceivable way that vaccination is anything less than the devil incarnate, but the simple truth is that once you understand the anatomy and physiology of the immune system, you realize that there has to be some benefit to the immune system from vaccination — by the simple act of introducing an antigen into the bloodstream. But you also realize what the limitations of that benefit are and also what dangers come with it. So let’s summarize.
 Vaccinations work on the same principles as natural immunity. If you introduce an antigen into the bloodstream, your immune system will mount a defense against it, and it will leave behind a memory of that defense. The strength of that response and the extent of that memory are variable, but on that simple principle alone, vaccinations must work — at least to some degree.
Vaccinations work on the same principles as natural immunity. If you introduce an antigen into the bloodstream, your immune system will mount a defense against it, and it will leave behind a memory of that defense. The strength of that response and the extent of that memory are variable, but on that simple principle alone, vaccinations must work — at least to some degree.- Any time you introduce an antigen into a human body — either naturally or by vaccination — it can have unexpected consequences. Some people have extreme reactions to the measles; some even die; most do not. Likewise, some people have extreme reactions to the measles vaccine; some even die; most do not. The problem is that it is much easier to focus blame when the harm is the result of a vaccination as opposed to an “act of God.”
- Vaccinations are not foolproof, but then neither is getting a disease naturally. Depending on how strong a response and memory are left behind from either antigen source, you will have strong immunity to a future occurrence of the disease…or little.
On the other hand!
- You are more likely to have a strong immune response to the disease itself for several reasons:
- Your body is exposed to “all” antigens presented by the disease, not just those extracted by the vaccine manufacturer.
- You are more likely to be sicker as a result of having had the actual disease (not necessarily a positive), thus your immune response and memory are likely to be stronger than that achieved through vaccination. There’s a tradeoff here.
- The strain of disease you are exposed to if you get the disease naturally will most likely be the most current strain circulating about. Most vaccines, other than the flu vaccine, are based on antigens that are quite old. Even flu vaccines, though, are based on last year’s viruses. The bottom line is that if your immunity comes from natural exposure to a current strain as opposed to an older strain in a vaccine, your immunity is more likely to be up to date and closer to that required as the disease continues to mutate over the years.
- Sometimes, there is more than one protein on a virus or bacteria that triggers an allergic response. If the protein fragment identified by researchers leaves out one or more of those components, the body’s response will be reduced, as will the subsequent immunity.
- Until recently, manufacturers had no option but to “grow” their vaccines in chicken eggs.9 James T. Matthews. “Egg-Based Production of Influenza Vaccine: 30 Years of Commercial Experience.” National Academy of Engineering. Fall 2006. <http://www.nae.edu/Publications/Bridge/EngineeringandVaccineProductionforanInfluenzaPandemic/Egg-BasedProductionofInfluenzaVaccine30YearsofCommercialExperience.aspx> ,10 Angelo DePalma, Ph.D. “Vaccine Development Aided by New Techniques.” Genetic Engineering & Biotechnology News. Nov 1, 2008 (Vol. 28, No. 19). <http://www.genengnews.com/gen-articles/vaccine-development-aided-by-new-techniques/2651/> Eggs are one of the most allergenic foods around. This significantly increased the chances of an unwanted “extra” reaction to the vaccine as opposed to natural exposure.
- Manufacturers add many substances to their vaccines. Thimerosal, a 49 percent mercury compound, which is used as a preservative in some vaccines, is the one most in the news, but you will also find additives such as ethylene glycol (antifreeze), formaldehyde (a known carcinogen), and aluminum as standard vaccine additives. At best, they have no health benefit. At worst, they are exactly as they sound — highly unhealthy. People in the natural health community accuse Thimerosal of causing autism. Scientists associated with governments, large pharmaceutical companies, and the mainstream medical community all cite a number of recent studies “proving” that there is no statistical correlation.11 Board on Population Health and Public Health Practice. “Immunization Safety Review: Thimerosal – Containing Vaccines and Neurodevelopmental Disorders.” 1 Oct 2001. INSTITUTE OF MEDICINE. <http://www.iom.edu/Reports/2001/Immunization-Safety-Review-Thimerosal—Containing-Vaccines-and-Neurodevelopmental-Disorders.aspx> ,12 Cristofer S. Price, William W. Thompson, Barbara Goodson, Eric S. Weintraub, et al. “Prenatal and Infant Exposure to Thimerosal From Vaccines and Immunoglobulins and Risk of Autism. 13 Sept 2010. Pediatrics. <http://pediatrics.aappublications.org/content/early/2010/09/13/peds.2010-0309.full.pdf> On the other hand, independent scientists tend to come to a different conclusion.13 José G. Dórea. “Integrating Experimental (In Vitro and In Vivo) Neurotoxicity Studies of Low-dose Thimerosal Relevant to Vaccines.” Neurochemical Research. Volume 36, Number 6, 927-938, DOI: 10.1007/s11064-011-0427-0. <http://www.springerlink.com/content/22115401745m3l44/> ,14 Olczak M, Duszczyk M, Mierzejewski P, Wierzba-Bobrowicz T, Majewska MD. “Lasting neuropathological changes in rat brain after intermittent neonatal administration of Thimerosal.” Folia Neuropathol. 2010;48(4):258-69. <http://www.ncbi.nlm.nih.gov/pubmed/21225508> My position on this is actually quite simple: I don’t really care whether Thimerosal causes autism or not. The simple fact is that mercury is one of the most toxic substances in nature, and it is a cumulative poison; the more you are exposed to it, the more it builds up in your body. The higher the levels in your body, the more the damage — and children are especially vulnerable. Anything that unnecessarily adds to that exposure is ipso facto unacceptable. There is simply no need, nor excuse, for its presence in vaccinations, amalgam fillings, or coal plant smokestacks. There! See how easy it is to sidestep the debate and cut to the heart of the matter.
- And finally, some scientists have made the case that by not allowing children to get many of the non-fatal diseases of childhood such as mumps, measles, and chicken pox, we have weakened their immune systems and made them much more vulnerable to far more dangerous “adult” versions of those same diseases. Or to look at it another way, vaccinations are like working out with a ten pound barbell to train your immune system. Allowing your body to experience the full disease is like working out with a 100 pound barbell.
As you can see, the story on vaccines is a mixed bag. I apologize to those of our readers who are upset that I did not categorically slam them, and I apologize to those on the other side of the debate who will be upset that I dismissed out of hand some of the shibboleths praising the safety and efficacy of vaccinations as dispensed to the media by governments and the mainstream medical community.
 I’m not saying vaccines should be eliminated, only that we should use more discrimination than we are at the moment. Eventually, it’s possible that new techniques of genetic engineering, by totally isolating the offending antigen, may be able to offer a safer and more effective form of vaccine. But for now, we need to remember that whatever benefit vaccines provide comes at a cost, and we need to decide, on a case by case basis, whether we wish to pay that cost.
I’m not saying vaccines should be eliminated, only that we should use more discrimination than we are at the moment. Eventually, it’s possible that new techniques of genetic engineering, by totally isolating the offending antigen, may be able to offer a safer and more effective form of vaccine. But for now, we need to remember that whatever benefit vaccines provide comes at a cost, and we need to decide, on a case by case basis, whether we wish to pay that cost.
Ultimately, the decision to vaccinate or not is a personal one — except where governments mandate the practice. And why do governments mandate vaccination? Yes, money and politics are involved, but in truth, most protectors of the establishment believe in Mr. Spock’s dictum from Star Trek (or John Stuart Mill for those who know better), “The needs of the many outweigh the needs of the few.” This is another way of saying that if your decision only affects you and your family, it’s your decision, but if your decision can provide a vehicle for a major “deadly” contagion to spread far and wide, then it becomes a community issue.
In our next issue the newsletter, we will conclude our series on the immune system by exploring:
- Potential problems for your immune system
- Antibiotics and antibiotic-resistant infections
- Natural pathogen destroyers
- Immunomodulators
- Specific recommendations for optimizing your immune system
Click below if you’ve missed any part of this Immunity series:
Anatomy and Physiology of the Immune System, Part 1
Anatomy and Physiology of the Immune System, Part 2
Anatomy and Physiology of the Immune System, Part 3
Anatomy and Physiology of the Immune System, Part 4
References
| ↑1 | Rus H, Cudrici C, Niculescu F (2005). “The role of the complement system in innate immunity”. Immunologic Research 33 (2): 103–12 <http://www.springerlink.com/content/d576088500r3x442/> |
|---|---|
| ↑2 | HOLGER KIRCHNER, MOSHE GLASER & RONALD B. HERBERMAN. “Suppression of cell-mediated tumour immunity by Corynebacterium parvum. Nature 257, 396 – 398 (02 October 1975). <http://www.nature.com/nature/journal/v257/n5525/abs/257396a0.html> |
| ↑3 | “BCG – the current vaccine for tuberculosis.” Initiative for Vaccine Research (IVR). World Health Organization. Accessed 7 Sept 2011. <http://www.who.int/vaccine_research/diseases/tb/vaccine_development/bcg/en/> |
| ↑4 | Charles Arthur, Technology Editor. “New strains of measles may resist vaccination.” 12 April 2001. Vaccination News. Accessed 9 Sept 2011. <http://www.vaccinationnews.com/Rally/NewMeaslesResist.htm> |
| ↑5 | Leslie Carol Botha. “SANE Vax Inc. Discovers Potential Bio-hazard Contaminant in Merck’s Gardasil™ HPV 4 Vaccine.” 12 September 2001. Sane Vax, Inc. Accessed 14 Sept 2011. <http://sanevax.org/sane-vax-inc-discovers-potential-bio-hazard-contaminant-in-merck%E2%80%99s-gardasil%E2%84%A2-hpv-4-vaccine-2/> |
| ↑6 | GordonT. Stewart. “VACCINATION AGAINST WHOOPING-COUGH : Efficacy versus Risks.” Volume 309, Lancet. Issue 8005, 29 January 1977, Pages 234-237 <http://www.sciencedirect.com/science/article/pii/S0140673677910285> |
| ↑7 | Roman Bystrianyk. “The Vaccine War: A Forgotten History.” 28 April 2010. I. http://www.healthsentinel.com/joomla/index.php?option=com_content&view=article&id=2752:the-vaccine-war-a-forgotten-history&catid=5:original&Itemid=24 |
| ↑8 | Update: Vaccine Side Effects, Adverse Reactions, Recommendations and Reports. “Contraindications, and Precautions Recommendations of the Advisory Committee on Immunization Practices (ACIP).” CDC September 06, 1996 / 45(RR-12);1-35. <http://www.cdc.gov/mmwr/preview/mmwrhtml/00046738.htm> |
| ↑9 | James T. Matthews. “Egg-Based Production of Influenza Vaccine: 30 Years of Commercial Experience.” National Academy of Engineering. Fall 2006. <http://www.nae.edu/Publications/Bridge/EngineeringandVaccineProductionforanInfluenzaPandemic/Egg-BasedProductionofInfluenzaVaccine30YearsofCommercialExperience.aspx> |
| ↑10 | Angelo DePalma, Ph.D. “Vaccine Development Aided by New Techniques.” Genetic Engineering & Biotechnology News. Nov 1, 2008 (Vol. 28, No. 19). <http://www.genengnews.com/gen-articles/vaccine-development-aided-by-new-techniques/2651/> |
| ↑11 | Board on Population Health and Public Health Practice. “Immunization Safety Review: Thimerosal – Containing Vaccines and Neurodevelopmental Disorders.” 1 Oct 2001. INSTITUTE OF MEDICINE. <http://www.iom.edu/Reports/2001/Immunization-Safety-Review-Thimerosal—Containing-Vaccines-and-Neurodevelopmental-Disorders.aspx> |
| ↑12 | Cristofer S. Price, William W. Thompson, Barbara Goodson, Eric S. Weintraub, et al. “Prenatal and Infant Exposure to Thimerosal From Vaccines and Immunoglobulins and Risk of Autism. 13 Sept 2010. Pediatrics. <http://pediatrics.aappublications.org/content/early/2010/09/13/peds.2010-0309.full.pdf> |
| ↑13 | José G. Dórea. “Integrating Experimental (In Vitro and In Vivo) Neurotoxicity Studies of Low-dose Thimerosal Relevant to Vaccines.” Neurochemical Research. Volume 36, Number 6, 927-938, DOI: 10.1007/s11064-011-0427-0. <http://www.springerlink.com/content/22115401745m3l44/> |
| ↑14 | Olczak M, Duszczyk M, Mierzejewski P, Wierzba-Bobrowicz T, Majewska MD. “Lasting neuropathological changes in rat brain after intermittent neonatal administration of Thimerosal.” Folia Neuropathol. 2010;48(4):258-69. <http://www.ncbi.nlm.nih.gov/pubmed/21225508> |








Interesting article. My wife
Interesting article. My wife has a staph infection in her spine and today she finished her last antibiotic treatment by way of a pick. If the antibiotics have not done their job, the doctor says they may have to operate on her spine. That’s the last thing we want. So I am very interested in any information that will allow her to combat the bacteria by building her immune system. Any help would be appreciated. She is in great pain and has been unable to work for nearly 3 months. It took 5 weeks just to get a diagnosis. It’s been horrible.
Great information on the
Great information on the immune system. I would like to add that the pharmaceutical industry has had over one-half a million lawsuits against them and is so unethical in so many ways. You are speaking from a scientic standpoint, the pharmaceutical industry is coming from greed and control over the healthcare system. They used ghost writers-made up studies, active placebos to make vaccines look good. Where drugs only treat the symptoms of disease, not the cause, not prevention, not to promote health, etc. So theory does not match their products. When drugs are needed in heroic medicine such as emergencies like an accident that is where it shines. However, all the war on pathogens will not create health. A healthy immune system and body will leave no place for pathogens to take root, we are already exposed to all of these pathogens. If the FDA (they said the 1st amendment did not apply to them) allowed free speech about supplements we would all be a lot healthier.
You traversed that mine field
You traversed that mine field well.
Your kind words warm the
Your kind words warm the cockles of my heart.
How do you balance out your
How do you balance out your immune system?
Is there anything we can do to control auto-immunity where the T Cells kill off pigment producing cells resulting in Vitiligo?
Hi Stan,
In part four of his
Hi Stan,
In part four of his series on the Immune System, Jon Barron will be addressing immunomodulators. Coming soon!
Your articles on the immune
Your articles on the immune system have been fantastic. I should not be surprised though, for I still use your 2005 Report on Aging (Vol2 Issue 2) as the ‘game-breaker’ that has turned my life around. You have the rare skill of explaining difficult concepts in a simple way and I cannot thank you enough for allowing me to share in your reports.
Best regards, Charles.
Dear Jon. Thank you for your
Dear Jon. Thank you for your continuing efforts to educate us. However . . . . >Or if it's been compromised by an HIV infection, it may not be able to muster a defense against tuberculosis.< With all due respect, Jon, 1) the existence of viruses has never been proven. 2) HIV is an allergy test and is being used to put the fear of AIDS into a persons mind, while there is no such thing as AIDS, other than a different way to apply VooDoo principles, through which peolpe are made sick and ultimately killed. 3) Tuberculosis bacteria in their inactive state are part and parcel of our immune system and a welcome addition to it. – When a 'cancer' tumour grows, the number of inactive TB bacteria grow at the same rate as the tumour grows, which grows as a result of a conflict shock event. Upon resolution of this biological conflict activity, the brain commands the TB bacteria to become active and they remove the tumour through a process called caseation. Therefore it is not wise to "fight" TB bacteria with anti-biotica, but realize that when they are active, the body is healing itself. There is one important proviso – one must consume extra protein to support the body's healing, because a lot of it gets excreted in this process. There is much more to discuss, but suffice this with an address to research more.
Dear Guest, you’re definitely
Dear Guest, you’re definitely persistent. You presented the same argument that “pathogenic viruses are a figment of the conventional medical establishment” in your comments to the last newsletter (http://www.jonbarron.org/immunity/anatomy-physiology-immune-system-b-cells). So, let us repeat Jon’s thoughts as he responded then.
Yes, Jon is familiar with the cell detritus theory; it is not new. It's roots go back to the 1920's with the work of Dr. Herbert Shelton and his disciple T.C. Fry. And as theories go, there is significantly more evidence that exists in support of the pathogenic virus theory than in support of the virus as cell detrius theory. If we are all around in another 50 years, we can compare notes and see which theory was finally validated.
Jon is also familiar with Dr. Hamer’s “conflict shock event” theory of cancer that proposes that cancer is the result of an emotional shock and the resulting stress and has addressed that before too. In his articles on cancer, he has certainly stated that both negative emotions and stress can play a role in causing the onset of cancer – both because of their impact on the immune system and their role in increasing production of free radicals — but do not logically figure to be cancer’s sole cause. Yes, conflict shock “might” explain the increase in cancer at Chernobyl, where people knew they had been exposed to radiation and were emotionally shocked by the information. But it does not explain the increase in cancer at Love Canal and in Erin Brokovich country, where people did not know they had been exposed to “carcinogens,” and therefore did not experience emotional shock – but got cancer nonetheless.
In the meantime, as Jon said, he can pretty much tell you that based on his 40 years of observations of tens of thousands of people who have used anti-pathogenic herbs to combat viruses (mythical though they may be), a significant percentage of them get well after using the herbs — even if it is just a figment of their imagination.
In any case, glad once again that you found the article interesting.
sir,
Iam a regular reader of
sir,
Iam a regular reader of your letters and know more about arthrities and glucosamine.one patient chronic rheumotoid arthrities having morepain in her knees and not walk even 10 meters for relief. I suggested glucosamine on first month.next month she take glucosamine with transferfactor(4life brand).now she walks more distance but pain is not reduce.Iwant to know
whether transfer factor is cure auto immune disorders suchas rheumotoid arthrities and others.?
whether she continue the same suppliments?
please send your valuable opinion
thank u
selvaraj
Hi Selvaraj, you may want to
Hi Selvaraj, you may want to check out: http://www.jonbarron.org/anti-aging/natural-health-topic-arthritis-remedies
Thanks for remembering the
Thanks for remembering the Trekkies!
SB, Kingston, ON
My pleasure!
My pleasure!
Thank you Jon Barron, Soo
Thank you Jon Barron, Soo informatve and really gave me insight to the true marvel of God’s creation. HUMAN BEINGS are made with everything in them to self cure along with thought. Who’s thought ,GOD’S.
DEAR JON: I´ve been reading
DEAR JON: I´ve been reading your letters since 2008, when my father got back for 2nd time retroperitoneal sarcoma (he passed away Dec.15 that year). I can tell you he was a very healthy guy before getting this very aggressive type of sarcoma. I agree with you very much in HAVING A HEALTHY LIFE STYLE, doesn´t guarantee you are not GETTING CANCER.
BUT I CAN TELL EVERYBODY MY FATHER HAD 76 VERY HEALTHY YEARS…before SARCOMA made it´s appeareance in his body.
He could run marathon´s in his sixties (years old)…AT 70 he decided to SLOW DOWN a little bit..only running 10 km and 20 km. He used to have a almost healthy diet, with natural fruits and vegetables, not too much MEAT…and probably MEAT WITHOUT HORMONES AND GRASS FED (HE LIVED IN VERACRUZ STATE, IN MEXICO…mostly all cows are grass fed)
BUT ON THE OTHER HAND HE PROBABLY HAD JUST A FEW VACCINE SHOTS…and due to his job (he was still active 6 months before his death) HE USED TO HAVE STREES IN HIS LIFE (2 JOBS) and he used to TRAVEL A LOT EXPOSED TO DIFFERENT PEOPLE, REGIONS AND LET´S SAYS VIRUS.
And I guess JOGGING, DANCING AND SINGING..was the way to PUT THAT STRESS OUT and that way not damaging a lot his IMMUNE SYSTEM.
SO YES…I AGREE THAT IT´S BETTER TO LEAD A HEALTHY LIFE (with some of the “sacrifices” that some people would say it implies)
This way eventhoug my father died of complications of his sarcoma,ALL AND ABSOLUTLY ALL HIS LIFE WAS HEALTHY, no arthritis, no knee problems, no diabetes, cholesterol,dementia etc…so he was a VERY ACTIVE person…so eventhough he wasn´t alive for 100 years..at least 76 was LIKE A YOUN ADULT (he also won some national and interntional championships…)
We don´t know for sure WHAT CAUSED HIS HIGH GRADE SARCOMA (MALIGNANT FIBROUS HYSTIOCITOMA)..perhaps SOME ENVIROMENTAL ISSUES DUE TO HIS MAIN JOB (OIL ENGINEER…HE COULD BE EXPOSED TO SOME CHEMICALS FOR SOME YEARS)…OR PERHAPS ONLY AGING.ANYWAY THANK YOU FOR ILUSTRATING ME!!! ELVIRA FROM MONTERREY, MEXICO
Hello, thank you for a
Hello, thank you for a thorough and scientific review of immune system function. I find this very helpful as we consider the possibilities of vaccinating our child (now 15 months old).
I wonder what you can tell me about the timing of maturation of the immune system and how that relates to the effectiveness and safety of vaccines. I have heard that vaccinating when children are young interferes with their ability to develop a strong immune system. Particularly because our daughter has some eczema, we want to wait until she is at least 2 before vaccinating, if we do decide to do this. Any information you can offer would be helpful.
Thank you again!
You did a good job in been
You did a good job in been unbiased but in the end the reader will most likely go against vaccines but even then gave good facts.